Bursa Foot Surgery Recuperation
Overview
Bursitis occurs when a bursa is irritated from frequent pressure and it becomes inflamed. Due to the location close the Achilles tendon, Achilles bursitis is often mistaken for tendinitis. Achilles bursitis is a common overuse injury in runners, ice skaters and other athletes.
Causes
Bursitis can develop for several reasons, including repetitively engaging in the same motion, or example, lifting objects above your head for work. Putting a lot of pressure on a bursa for an extended period of time. Leaning on your elbows or kneeling (for example, to lay carpet) can cause bursitis in the elbows or knees. If you sit for long periods of time, especially on hard surfaces, you may develop bursitis in your hip. Wearing shoes with a stiff back that rubs against the back of the ankle can cause Achilles tendon bursitis. Trauma. The bursae at the knee and elbow are close to the surface of the skin, and if you fall directly on your elbow or the knee, you can rupture, injure or puncture a bursa. Infection. Known as septic bursitis, it?s the result of bacteria infecting a bursa. It can occur from an infection traveling from another site or following an accident that ruptures the bursa. Even scraping the skin on your elbow or getting a mosquito bite that breaks the skin near the olecranon bursa (near the elbow) can lead to bursitis. Other joint disorders, such as rheumatoid arthritis, osteoarthritis and gout, or health conditions.
Symptoms
The main symptom of heel bursitis is pain. You may experience pain in your heel when you walk or run. There may also be pain if the area is touched or if you stand on your tiptoes. In addition to pain, the area may appear red and warm, which are both signs of inflammation. Even if you have these symptoms, only a doctor can determine if you have bursitis of the heel. Your doctor will use these symptoms along with a general exam to determine if you are suffering from bursitis of the heel.
Diagnosis
During the physical examination of a patient with calcaneal bursitis, the physician should keep the following considerations in mind. Swelling and redness of the posterior heel (the pump bump) may be clearly apparent. The inflamed area, which may be slightly warm to the touch, is generally tender to palpation. Careful examination can help the clinician to distinguish whether the inflammation is posterior to the Achilles tendon (within the subcutaneous calcaneal bursa) or anterior to the tendon (within the subtendinous calcaneal bursa). Differentiating Achilles tendinitis/tendinosis from bursitis may be impossible. At times, the 2 conditions co-exist. Isolated subtendinous calcaneal bursitis is characterized by tenderness that is best isolated by palpating just anterior to the medial and lateral edges of the distal Achilles tendon. Conversely, insertional Achilles tendinitis is notable for tenderness that is located slightly more distally, where the Achilles tendon inserts on the posterior calcaneus. A patient with plantar fasciitis has tenderness along the posterior aspect of the sole, but he/she should not have tenderness with palpation of the posterior heel or ankle. A patient with a complete avulsion or rupture of the Achilles tendon demonstrates a palpable defect in the tendon, weakness in plantarflexion, and a positive Thompson test on physical examination. During the Thompson test, the examiner squeezes the calf. The test is negative if this maneuver results in passive plantarflexion of the ankle, which would indicate that the Achilles tendon is at least partially intact.
Non Surgical Treatment
The most important factor in healing bursitis is resting your foot and ankle. This can be difficult when you have to carry on with daily activities, but resting and elevating your foot whenever you can is recommended. During your recovery you will probably have to modify or avoid the activities that stress your bursa until your pain and inflammation settle.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Prevention
Once your pain and inflammation is gone, you can prevent retrocalcaneal bursitis deformity by wearing the best shoes for your foot type. You should high-heels and pumps if possible. Wear orthotics (custom arch supports) or over-the-counter orthotic devices. Perform frequent Achilles tendon stretching exercises to prevent it from becoming tight agian. Avoiding running uphill when training. Try to run on softer surfaces and avoid concrete.
Bursitis occurs when a bursa is irritated from frequent pressure and it becomes inflamed. Due to the location close the Achilles tendon, Achilles bursitis is often mistaken for tendinitis. Achilles bursitis is a common overuse injury in runners, ice skaters and other athletes.
Causes
Bursitis can develop for several reasons, including repetitively engaging in the same motion, or example, lifting objects above your head for work. Putting a lot of pressure on a bursa for an extended period of time. Leaning on your elbows or kneeling (for example, to lay carpet) can cause bursitis in the elbows or knees. If you sit for long periods of time, especially on hard surfaces, you may develop bursitis in your hip. Wearing shoes with a stiff back that rubs against the back of the ankle can cause Achilles tendon bursitis. Trauma. The bursae at the knee and elbow are close to the surface of the skin, and if you fall directly on your elbow or the knee, you can rupture, injure or puncture a bursa. Infection. Known as septic bursitis, it?s the result of bacteria infecting a bursa. It can occur from an infection traveling from another site or following an accident that ruptures the bursa. Even scraping the skin on your elbow or getting a mosquito bite that breaks the skin near the olecranon bursa (near the elbow) can lead to bursitis. Other joint disorders, such as rheumatoid arthritis, osteoarthritis and gout, or health conditions.
Symptoms
The main symptom of heel bursitis is pain. You may experience pain in your heel when you walk or run. There may also be pain if the area is touched or if you stand on your tiptoes. In addition to pain, the area may appear red and warm, which are both signs of inflammation. Even if you have these symptoms, only a doctor can determine if you have bursitis of the heel. Your doctor will use these symptoms along with a general exam to determine if you are suffering from bursitis of the heel.
Diagnosis
During the physical examination of a patient with calcaneal bursitis, the physician should keep the following considerations in mind. Swelling and redness of the posterior heel (the pump bump) may be clearly apparent. The inflamed area, which may be slightly warm to the touch, is generally tender to palpation. Careful examination can help the clinician to distinguish whether the inflammation is posterior to the Achilles tendon (within the subcutaneous calcaneal bursa) or anterior to the tendon (within the subtendinous calcaneal bursa). Differentiating Achilles tendinitis/tendinosis from bursitis may be impossible. At times, the 2 conditions co-exist. Isolated subtendinous calcaneal bursitis is characterized by tenderness that is best isolated by palpating just anterior to the medial and lateral edges of the distal Achilles tendon. Conversely, insertional Achilles tendinitis is notable for tenderness that is located slightly more distally, where the Achilles tendon inserts on the posterior calcaneus. A patient with plantar fasciitis has tenderness along the posterior aspect of the sole, but he/she should not have tenderness with palpation of the posterior heel or ankle. A patient with a complete avulsion or rupture of the Achilles tendon demonstrates a palpable defect in the tendon, weakness in plantarflexion, and a positive Thompson test on physical examination. During the Thompson test, the examiner squeezes the calf. The test is negative if this maneuver results in passive plantarflexion of the ankle, which would indicate that the Achilles tendon is at least partially intact.
Non Surgical Treatment
The most important factor in healing bursitis is resting your foot and ankle. This can be difficult when you have to carry on with daily activities, but resting and elevating your foot whenever you can is recommended. During your recovery you will probably have to modify or avoid the activities that stress your bursa until your pain and inflammation settle.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Prevention
Once your pain and inflammation is gone, you can prevent retrocalcaneal bursitis deformity by wearing the best shoes for your foot type. You should high-heels and pumps if possible. Wear orthotics (custom arch supports) or over-the-counter orthotic devices. Perform frequent Achilles tendon stretching exercises to prevent it from becoming tight agian. Avoiding running uphill when training. Try to run on softer surfaces and avoid concrete.
Non Surgical Hammer Toe Repair
 Overview
Overview
A hammertoes is a misshapen second, third, or fourth toe. The toe bends up at the middle joint. The toe becomes a hammertoe because a muscle in the toe isn?t working properly or is too weak, increasing pressure on the tendons and the toe joints. Muscles normally work in twos to bend and straighten toes. If the toe stays bent too long, a hammertoe develops. Ill-fitting shoes, arthritis, heredity, even an injury, can cause the hammertoe to form. To add insult to injury, corns and calluses are common on top of hammertoes because the toe is rubbing against the shoe.
Causes
Hammertoe has three main culprits: tight shoes, trauma, and nerve injuries or disorders. When toes are crowded in shoes that are too tight and narrow, they are unable to rest flat, and this curled toe position may become permanent even when you aren't wearing shoes due to the tendons of the toe permanently tightening. When the tendons are held in one position for too long, the muscles tighten and eventually become unable to stretch back out. A similar situation may result when tendons are injured due to trauma, such as a stubbed, jammed, or broken toe.
 Symptoms
Symptoms
Symptoms of a hammertoe are usually first noticed as a corn on the top of the toe or at the tip which produces pain with walking or wearing tight shoes. Most people feel a corn is due to a skin problem on their toes, which in fact, it is Hammer toe protecting the underlying bone deformity. A corn on the toe is sometimes referred to as a heloma dura or heloma durum, meaning hard corn. This is most common at the level of the affected joint due to continuous friction of the deformity against your shoes.
Diagnosis
Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred.
Non Surgical Treatment
The treatment options vary with the type and severity of each hammertoe, although identifying the deformity early in its development is important to avoid surgery. Podiatric medical attention should be sought at the first indication of pain and discomfort because, if left untreated, hammertoes tend to become rigid, making a nonsurgical treatment less of an option. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Surgical Treatment
If conservative measures fail to provide relief, or if your hammertoe is in advanced stages with rigidity and a significant amount of pain, surgery may be required. Some patients also require surgery if they have open sores or wounds related to their hammertoe. For patients who also suffer from bunions, a combined procedure may be appropriate, addressing both conditions within the same surgery. Recovery time will vary from patient to patient, depending on the extent of the surgical repair and other conditions that may also be present.
 Prevention
Prevention
In some cases foot problems may present at birth, many foot problems such as hammer toes can be prevented. Hammer toe prevention can be a simple process, such as, checking your feet regularly and wearing the right shoes for your feet. Good circulation is also an essential part of foot health and hammer toe prevention. Taking a warm foot bath or giving yourself a foot massage are great ways of keeping your feet healthy.
Hammertoe Pain Treatment
 Overview
Overview
Hammer, claw, and mallet toes are toes that do not have the right shape. They may look odd or may hurt, or both. Tight shoes are the most common cause of these toe problems. A hammertoes is a toe that bends down toward the floor at the middle toe joint. It usually happens in the second toe. This causes the middle toe joint to rise up. Hammer toes often occur with bunions. Claw toe often happens in the four smaller toes at the same time. The toes bend up at the joints where the toes and the foot meet. They bend down at both the middle joints and at the joints nearest the tip of the toes. This causes the toes to curl down toward the floor. A mallet toe often happens to the second toe, but it may happen in the other toes as well. The toe bends down at the joint closest to the tip of the toe.
Causes
Hammer toe may also be caused by other medical conditions such as rheumatoid arthritis, osteoarthritis, or stroke because these forms of illnesses involve affectation of the person's muscles and nerves. Diabetes is also a causative factor for hammer toes due to diabetic neuropathy, which often times accompanies advanced instances of diabetes. Injury to a person's toes may also cause hammer toes, particularly if the injury involves breaking of the toes. In some instances, hammer toes may be hereditary. Some people may be genetically predisposed to develop the condition because of the natural structure of their bodies.
 Symptoms
Symptoms
Common reasons patients seek treatment for toe problems are toe pain on the knuckle. Thick toe calluses. Interference with walking/activities. Difficulty fitting shoes. Worsening toe deformity. Pain at the ball of the foot. Unsightly appearance. Toe deformities (contractures) come in varying degrees of severity, from slight to severe. The can be present in conjunction with a bunion, and develop onto a severe disfiguring foot deformity. Advanced cases, the toe can dislocate on top of the foot. Depending on your overall health, symptoms and severity of the hammer toe, the condition may be treated conservatively and/or with surgery.
Diagnosis
The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position.
Non Surgical Treatment
A toe doctor can provide you with devices such as hammer toe regulators or straighteners. These are also available for purchase locally. Another good idea is to start the hammer toe rehabilitation process by gently trying to straighten the joint and moving and flexing the affected toe as much as possible without straining it. If hammer toe taping doesn?t work, you may require surgery. If the joints and tendons have stiffened to a point of non-movement, hammer toe corrective surgery may need to enter the toe and either cut or manually move some of the tendons and ligaments. Although the treatment is relatively safe fast, you may deal with some stiffness afterwards.
Surgical Treatment
The technique the surgeon applies during the surgery depends on how much flexibility the person's affected toes still retain. If some flexibility has still been preserved in their affected toes, the hammer toes might be corrected through making a small incision into the toe so the surgeon can manipulate the tendon that is forcing the person's toes into a curved position. If, however, the person's toes have become completely rigid, the surgeon might have to do more than re-aligning the person's tendons. Some pieces of bone may have to be removed so the person's toe has the ability to straighten out. If this is the case, some pins are attached onto the person's foot afterwards hammertoes to fix their bones into place while the injured tissue heals.
The Facts Related To Overpronation Of The Feet
Overview
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Overpronation may have secondary effects on the lower legs, such as increased rotation of the tibia, which may result in lower leg or knee problems. Overpronation is usually associated with many overuse injuries in running including medial tibial stress syndrome, or shin splints, and knee pain Individuals with injuries typically have pronation movement that is about two to four degrees greater than that of those with no injuries. Between 40% and 50% of runners who overpronate do not have overuse injuries. This suggests that although pronation may have an effect on certain injuries, it is not the only factor influencing their development.
Diagnosis
Do the wet foot test. Get your feet wet and walk along a paved surface or sand and look at the footprints you leave. If you have neutral feet you will see a print of the heel with a thin strip connecting to your forefoot, but if you're overpronating your foot print will look a bit like a giant blob with toes.
Non Surgical Treatment
Adequate footwear can often help with conditions related to flat feet and high arches. Certified Pedorthists recommend selecting shoes featuring heel counters that make the heel of the shoe stronger to help resist or reduce excessive rearfoot motions. The heel counter is the hard piece in the back of the shoe that controls the foot?s motion from side-to-side. You can quickly test the effectiveness of a shoe?s heel counter by placing the shoe in the palm of your hand and putting your thumb in the mid-portion of the heel, trying to bend the back of the shoe. A heel counter that does not bend very much will provide superior motion control. Appropriate midsole density, the firmer the density, the more it will resist motion (important for a foot that overpronates or is pes planus), and the softer the density, the more it will shock absorb (important for a cavus foot with poor shock absorption) Wide base of support through the midfoot, to provide more support under a foot that is overpronated or the middle of the foot is collapsed inward.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Over-pronation, or flat feet, is a common biomechanical problem that occurs in the walking process when a person?s arch collapses upon weight bearing. This motion can cause extreme stress or inflammation on the plantar fascia, possibly causing severe discomfort and leading to other foot problems.
Causes
You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation.
Symptoms
Overpronation may have secondary effects on the lower legs, such as increased rotation of the tibia, which may result in lower leg or knee problems. Overpronation is usually associated with many overuse injuries in running including medial tibial stress syndrome, or shin splints, and knee pain Individuals with injuries typically have pronation movement that is about two to four degrees greater than that of those with no injuries. Between 40% and 50% of runners who overpronate do not have overuse injuries. This suggests that although pronation may have an effect on certain injuries, it is not the only factor influencing their development.
Diagnosis
Do the wet foot test. Get your feet wet and walk along a paved surface or sand and look at the footprints you leave. If you have neutral feet you will see a print of the heel with a thin strip connecting to your forefoot, but if you're overpronating your foot print will look a bit like a giant blob with toes.
Non Surgical Treatment
Adequate footwear can often help with conditions related to flat feet and high arches. Certified Pedorthists recommend selecting shoes featuring heel counters that make the heel of the shoe stronger to help resist or reduce excessive rearfoot motions. The heel counter is the hard piece in the back of the shoe that controls the foot?s motion from side-to-side. You can quickly test the effectiveness of a shoe?s heel counter by placing the shoe in the palm of your hand and putting your thumb in the mid-portion of the heel, trying to bend the back of the shoe. A heel counter that does not bend very much will provide superior motion control. Appropriate midsole density, the firmer the density, the more it will resist motion (important for a foot that overpronates or is pes planus), and the softer the density, the more it will shock absorb (important for a cavus foot with poor shock absorption) Wide base of support through the midfoot, to provide more support under a foot that is overpronated or the middle of the foot is collapsed inward.
Prevention
Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise.
Calf stretch:Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times.
Golf ball:While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds.
Big toe push: Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions.
Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times.
Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Bunions Cause And Effect
Overview
 Bunions (hallux valgus) are often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. With a bunion, the big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion's "bump." Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which continues to become increasingly prominent. Bunions can be painful, but not always. Bunions are always progressive, so the deformity becomes more prounced over time, even if its not painful.
Bunions (hallux valgus) are often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. With a bunion, the big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion's "bump." Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which continues to become increasingly prominent. Bunions can be painful, but not always. Bunions are always progressive, so the deformity becomes more prounced over time, even if its not painful.
Causes
Bunions may be hereditary, as they often run in families. This suggests that people may inherit a faulty foot shape. In addition, footwear that does not fit properly may cause bunions. Bunions are made worse by tight, poorly-fitting, or too-small shoes. Bunions may also happen due to inflammatory conditions such as arthritis. Anyone can get bunions, but they are more common in women. People with flat feet are also more likely to get bunions due to the changes in the foot caused by bunions. There is also a condition called adolescent bunion, which tends to occur in 10-to-15-year old girls.
Symptoms
It is unusual to have much bunion or hallux valgus pain when out of shoe wear or at rest. There are exceptions to this and in particular if symptoms have been ignored during the day and the bunion has become very painful during the day then some symptoms may be present at night. The pain from the region of the great toe at rest or at night is however more often a symptom of an arthritic big toe (hallux rigidus) rather than a straightforward bunion. To confuse matters these two conditions can sometimes coexist. Bunion or hallux valgus pain is most often present when walking in enclosed shoes. There may be little bunion pain in sandals or barefoot. It is unusual to have much bunion pain when not putting weight on the foot or at night. If there is bunion pain at rest or at night then there may also be arthritic change within the toe.
Diagnosis
People with bunions may be concerned about the changing appearance of their feet, but it is usually the pain caused by the condition that leads them to consult their doctor. The doctor will evaluate any symptoms experienced and examine the affected foot for joint enlargement, tissue swelling and/or tenderness. They will also assess any risk factors for the condition and will ask about family history. An x-ray of the foot is usually recommended so that the alignment of big toe joint can be assessed. This would also allow any other conditions that may be affecting the joint, such as arthritis, to be seen.
Non Surgical Treatment
There are a number of treatment options for bunions. Non-surgical treatments are usually tried first, including painkillers, orthotics (insoles) and bunion pads. However, these can only help to reduce the symptoms of bunions, such as pain. They don't improve the appearance of your foot. 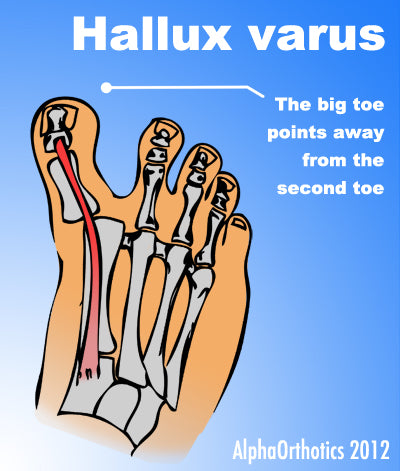
Surgical Treatment
If the bunion symptoms does not respond to the conservative measures or if the bunion has progressed past a threshold where these measures are not effective, bunion surgery may be necessary to correct alignment and remove the bunion. A large range of types of surgical procedures for bunions are available and the choice will depend on things like what bone or bones are involved, the angular relationship between the different bones, the amount of damage to the joint and the presence of deformities other than the bunion.
Does Severs Disease Require Surgical Treatments?
Overview
n the growing child there are a number of different ways that bones grow. In the calcaneus (heel bone), growth comes from two separate growth plates. The lesser of the two growth plates is called the apophysis. The apophysis of the calcaneus is located between the back and the bottom of the heel at that spot that hits the ground each time we take a step. The Achilles tendon, which is the most powerful tendons in our body, attaches to the proximal aspect of the apophysis. The plantar fascia attaches to the distal aspect of the apophysis. Both the Achilles tendon and plantar fascia place traction, or pulling on the growth plate and contribute to inflammation of the secondary growth plate called apophysitis. The calcaneal apophysis is very apparent on x-ray and continues to grow until approximately age 12 in girls and age 15 in boys.
Causes
Sever?s disease only occurs during a certain period of pre-adolescence, when the heel bone is going through a rapid growth spurt. In girls, this typically occurs around 8 to 10 years of age, and in boys, between ages 10 and 13. Sever?s disease is more common in active, athletic children. The condition is difficult to prevent completely, but changing the type and amount of physical activity when your child is experiencing pain will help.
Symptoms
Severs causes swelling, pain and tenderness over the back of the heel. Your child may walk with a limp. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. The swelling increases and is painful when touched or knocked. It commonly affects boys who are having a growth spurt during their pre-teen or teenage years. One or both knees may be affected.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
The treatment of Sever's disease depends upon the severity of symptoms experienced by the patient. Care is initiated with a simple program of stretching and heel elevation to weaken the force applied to the calcaneus by the Achilles tendon. If stretches and heel elevation are unsuccessful in controlling the symptoms of Sever's disease, children should be removed from sports and placed on restricted activities. Mild Symptoms. Wear a 3/8 heel lift at all times (not just during physical activity). It is important to use a firm lift and not a soft heel pad. Calf stretches 6/day for 60 seconds each. Calf stretches are best accomplished by standing with the toes on the edge of a stretching block. Moderate Symptoms. Follow the directions for minor symptoms and decrease activity including elimination of any athletic activity. In addition to stretching by day, a night stretching splint can be worn while sleeping. Severe Symptoms. Follow the directions for mild and moderate symptoms. Children should be removed from sports activities such as football, basketball, soccer or gym class. A below knee walking cast with a heel lift or in severe cases, non-weight bearing fiberglass cast, may be indicated for 4-6 weeks. The cast should be applied in a mildly plantar flexed position. Cam Walkers should not be used for Sever's Disease unless they have a built in heel lift.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
n the growing child there are a number of different ways that bones grow. In the calcaneus (heel bone), growth comes from two separate growth plates. The lesser of the two growth plates is called the apophysis. The apophysis of the calcaneus is located between the back and the bottom of the heel at that spot that hits the ground each time we take a step. The Achilles tendon, which is the most powerful tendons in our body, attaches to the proximal aspect of the apophysis. The plantar fascia attaches to the distal aspect of the apophysis. Both the Achilles tendon and plantar fascia place traction, or pulling on the growth plate and contribute to inflammation of the secondary growth plate called apophysitis. The calcaneal apophysis is very apparent on x-ray and continues to grow until approximately age 12 in girls and age 15 in boys.
Causes
Sever?s disease only occurs during a certain period of pre-adolescence, when the heel bone is going through a rapid growth spurt. In girls, this typically occurs around 8 to 10 years of age, and in boys, between ages 10 and 13. Sever?s disease is more common in active, athletic children. The condition is difficult to prevent completely, but changing the type and amount of physical activity when your child is experiencing pain will help.
Symptoms
Severs causes swelling, pain and tenderness over the back of the heel. Your child may walk with a limp. Initially the pain may be intermittent occurring only during or after exercise. As the problem gets worse, pain may be present most of the time. The swelling increases and is painful when touched or knocked. It commonly affects boys who are having a growth spurt during their pre-teen or teenage years. One or both knees may be affected.
Diagnosis
A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
The treatment of Sever's disease depends upon the severity of symptoms experienced by the patient. Care is initiated with a simple program of stretching and heel elevation to weaken the force applied to the calcaneus by the Achilles tendon. If stretches and heel elevation are unsuccessful in controlling the symptoms of Sever's disease, children should be removed from sports and placed on restricted activities. Mild Symptoms. Wear a 3/8 heel lift at all times (not just during physical activity). It is important to use a firm lift and not a soft heel pad. Calf stretches 6/day for 60 seconds each. Calf stretches are best accomplished by standing with the toes on the edge of a stretching block. Moderate Symptoms. Follow the directions for minor symptoms and decrease activity including elimination of any athletic activity. In addition to stretching by day, a night stretching splint can be worn while sleeping. Severe Symptoms. Follow the directions for mild and moderate symptoms. Children should be removed from sports activities such as football, basketball, soccer or gym class. A below knee walking cast with a heel lift or in severe cases, non-weight bearing fiberglass cast, may be indicated for 4-6 weeks. The cast should be applied in a mildly plantar flexed position. Cam Walkers should not be used for Sever's Disease unless they have a built in heel lift.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
What Is Adult Aquired FlatFeet ?
Overview
Adult-acquired flatfoot (AAF) is the term used to describe the progressive deformity of the foot and ankle that, in its later stages, results in collapsed and badly deformed feet. Although the condition has been described and written about since the 1980s, AAF is not a widely used acronym within the O&P community-even though orthotists and pedorthists easily recognize the signs of the condition because they treat them on an almost daily basis. AAF is caused by a loss of the dynamic and static support structures of the medial longitudinal arch, resulting in an incrementally worsening planovalgus deformity associated with posterior tibial (PT) tendinitis. Over the past 30 years, researchers have attempted to understand and explain the gradual yet significant deterioration that can occur in foot structure, which ultimately leads to painful and debilitating conditions-a progression that is currently classified into four stages. What begins as a predisposition to flatfoot can progress to a collapsed arch, and then to the more severe posterior tibial tendon dysfunction (PTTD). Left untreated, the PT tendon can rupture, and the patient may then require a rigid AFO or an arthrodesis fixation surgery to stabilize the foot in order to remain capable of walking pain free. 
Causes
The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction. What causes adult acquired flat foot? Fracture or dislocation. Tendon laceration. Tarsal Coalition. Arthritis. Neuroarthropathy. Neurological weakness.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. Asymmetrical collapsing of the medial arch on the affected side.
Diagnosis
Your podiatrist is very familiar with tendons that have just about had enough, and will likely be able to diagnose this condition by performing a physical exam of your foot. He or she will probably examine the area visually and by feel, will inquire about your medical history (including past pain or injuries), and may also observe your feet as you walk. You may also be asked to attempt standing on your toes. This may be done by having you lift your ?good? foot (the one without the complaining tendon) off the ground, standing only on your problem foot. (You may be instructed to place your hands against the wall to help with balance.) Then, your podiatrist will ask you to try to go up on your toes on the bad foot. If you have difficulty doing so, it may indicate a problem with your posterior tibial tendon. Some imaging technology may be used to diagnose this condition, although it?s more likely the doctor will rely primarily on a physical exam. However, he or she may order scans such as an MRI or CT scan to look at your foot?s interior, and X-rays might also be helpful in a diagnosis.
Non surgical Treatment
In the early stages, simple pre-fabricated orthotics can help improve the heel position to reduce the mechanical load which is contributing to the symptoms. In advanced stages or long term orthotic use, a plaster of paris or foam box cast can be taken and specific bespoke orthotics manufactured. If the condition develops further a AFO (ankle foot orthotic) may be necessary for greater control. In more advanced stages of symptomatic Adult Acquired flat feet, where the conservative methods of treatment have failed there are various forms of surgery available depending upon the root cause of the issue and severity. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.